Progress and Thinking of CAR-T for DLBCL Treatment
Progress and Thinking of CAR-T for DLBCL Treatment
Exploration never stops, and the grand meeting is just around the corner. From January 26 to 28, 2024, the “Working Conference of the Leukemia Expert Committee, Lymphoma Expert Committee, and Myeloma Preparatory Committee of the Chinese Society of Clinical Oncology (CSCO), and the 2024 CSCO Academic Conference on Hematological and Lymphoid Malignancies and Myeloma” was held in the beautiful city of Haikou, Hainan Province. Renowned experts and scholars from home and abroad gathered to share and exchange the latest advancements and hot topics in the field of hematological malignancies. At the meeting, Professor Zou Dehui from the Lymphoma Diagnosis and Treatment Center of the Chinese Academy of Medical Sciences Blood Disease Hospital (Chinese Academy of Medical Sciences Institute of Hematology) delivered a presentation titled “Progress and Reflections on CAR-T Therapy for B-Cell Lymphoma,” sharing the latest research progress on the efficacy, therapeutic position, challenges, and optimization strategies of CAR-T therapy for diffuse large B-cell lymphoma (DLBCL). This journal has specially compiled the following content.

Efficacy of CAR-T Therapy: Further Evidence of Cure Potential
In recent years, CD19-targeted CAR-T cell therapy has achieved tremendous success in the field of B-cell non-Hodgkin’s lymphoma (B-NHL). Currently, several anti-CD19 CAR-T cell therapy drugs have been approved for domestic and international use in patients with relapsed/refractory (R/R) large B-cell lymphoma (LBCL) who have received ≥2 lines of treatment, including Axicabtagene Ciloleucel (Axi-cel), Tis-cel, Liso-cel, and Relmacabtagene Autoleucel (Relma-cel), among which Axi-cel and Relma-cel were approved for marketing in China in June and September 2021, respectively.
The pivotal clinical trials ZUMA-1, JULIET, and TRANSCEND NHL001 have previously demonstrated that Axi-cel, Tis-cel, and Liso-cel can significantly improve the overall survival (OS) and progression-free survival (PFS) rates of DLBCL patients. The latest 6-year follow-up results of the ZUMA-1 study, presented at the 2023 American Society of Hematology (ASH) annual meeting, further showed that among the 59 patients who achieved the best complete response (bCR) after Axi-cel treatment, the 5-year duration of complete response (DOCR) rate reached 56.7%, and for patients who maintained CR for 12 months and 24 months, the 5-year DOCR rates were as high as 84.3% and 91.3%, respectively, demonstrating the potential for cure. Similarly, the 2-year follow-up results for Relma-cel presented at the 2022 American Society of Clinical Oncology (ASCO) annual meeting were equally encouraging, with a median duration of response (DOR) of 20.3 months and a 2-year DOR rate of 40.3%. In the commercial dose group (100×106 dose group), the median DOR was 23.3 months, and the 2-year DOR rate reached 56.18%.
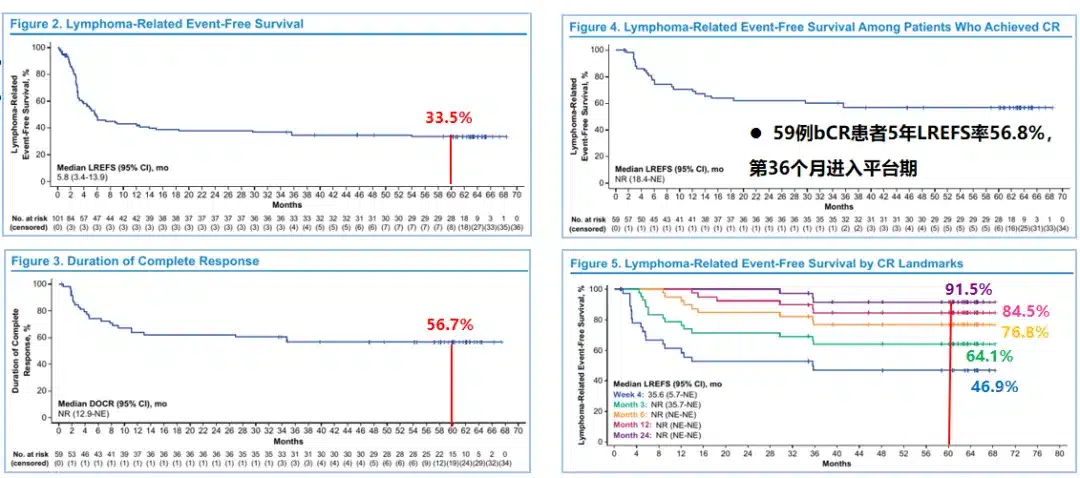
△ 6-year follow-up results of the ZUMA-1 study
Furthermore, the 2023 ASH annual meeting also presented the results of two real-world studies (RWS) on Axi-cel. One was an RWS from the U.S. Lymphoma CAR-T Consortium, which showed that the 5-year OS rate for Axi-cel treatment of R/R LBCL patients was as high as 40.3%, confirming the consistency between the real-world efficacy and the registration study. Although the study included 43% of patients who did not meet the ZUMA-1 study criteria, 29% of patients remained in continuous remission at a median follow-up of 58 months. The other was the first RWS conducted in the Chinese population, whose interim analysis showed a median DOR of 13.7 months for Axi-cel treatment of R/R NHL; the median DOR was not reached for bCR patients, while for patients with a best response of partial remission (PR), the median DOR was 4.7 months; the median PFS was 14.6 months; the median OS was not reached, with an estimated 12-month OS rate of 80.4%. Additionally, no new adverse events were observed in Chinese subjects.
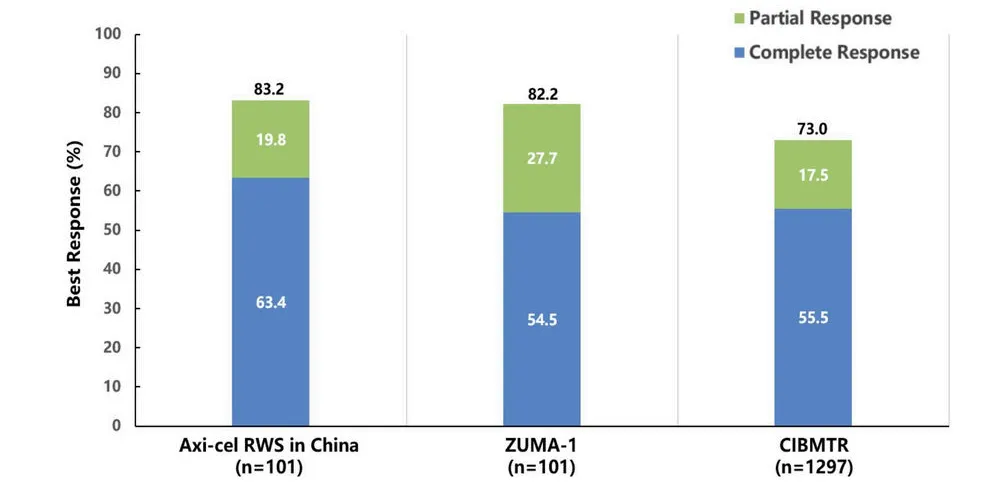
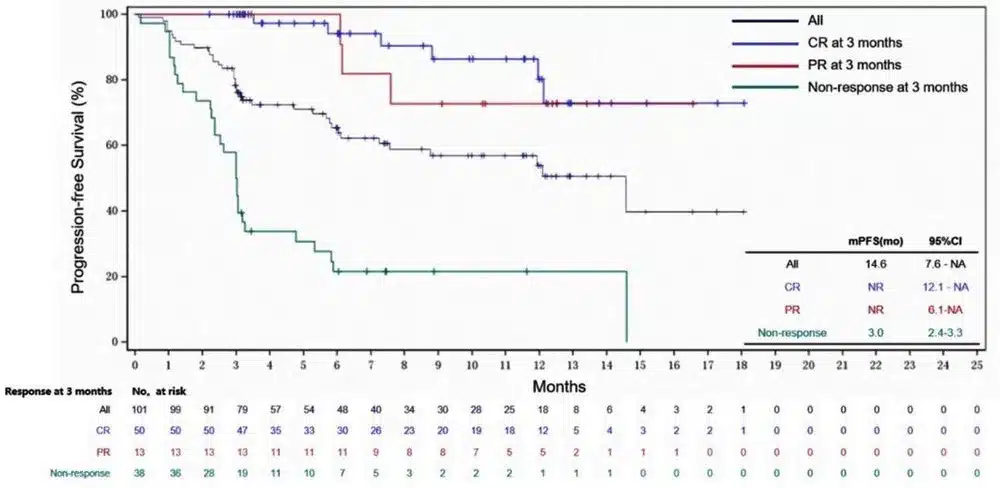
△ Interim analysis of the real-world study of Axi-cel for the treatment of R/R NHL in China
Therapeutic Position of CAR-T: Established in Third-Line, Challenging Second-Line
As CAR-T therapy is increasingly applied in clinical settings, various factors influencing its efficacy have been discovered, one of which is the number of treatment lines. Real-world data presented at the 2022 European Hematology Association (EHA) annual meeting showed that as the number of treatment lines increased, the complete response (CR) rate and survival outcomes of CAR-T therapy for R/R DLBCL decreased. At the 2023 ASH annual meeting, a multicenter retrospective propensity score-matched analysis from Iran included 44 LBCL patients who received Axi-cel treatment between January 2019 and June 2023, with 22 patients in the second-line and 22 in the third-line treatment groups. The results showed that second-line Axi-cel treatment had a higher objective response rate (ORR) and PFS compared to third-line treatment, while the incidence of adverse events (AEs) was similar. Higher CAR-T expansion in the second-line treatment suggested that the CAR-T product prepared at an earlier line had better quality and a more favorable T-cell subtype composition.
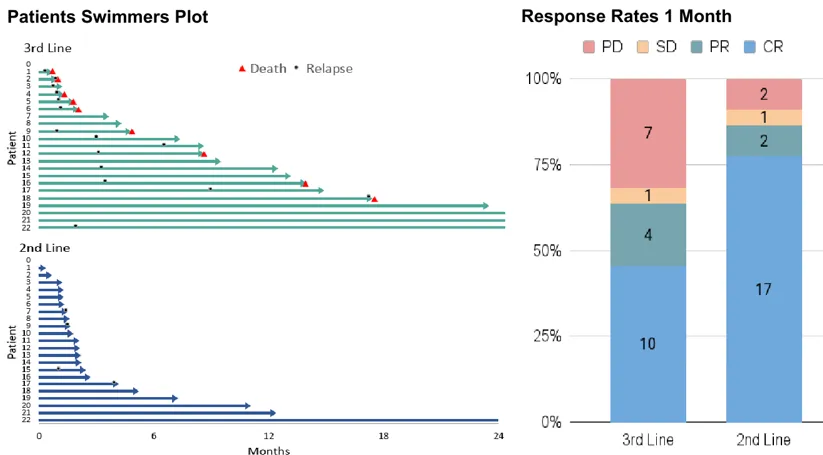
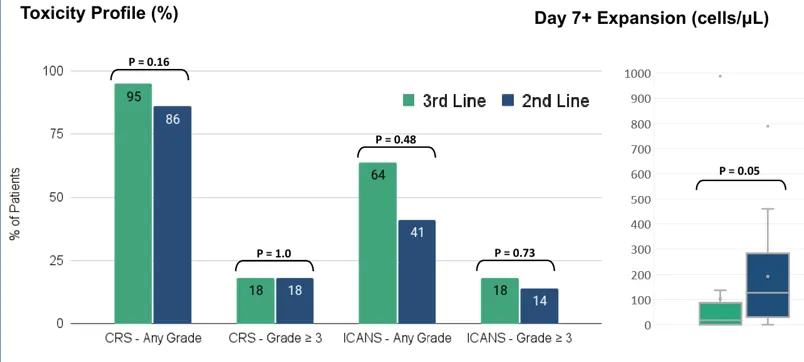
△ Multicenter retrospective propensity score-matched analysis from Iran
Based on these findings and the outstanding performance of CAR-T therapy in DLBCL, multiple phase III clinical trials of CAR-T have begun challenging the standard of care (SOC) in the second-line setting, but consistent results have yet to be achieved. The ZUMA-7 and TRANSFORM studies showed that compared to SOC, Axi-cel significantly improved event-free survival (EFS) [HR (95% CI) of 0.4 (0.31-0.51) and 0.35 (0.23-0.53), respectively], while the Belinda study showed no significant improvement in EFS with Axi-cel compared to SOC [HR (95% CI) of 1.07 (0.82-1.4)], although this study has not yet reached its primary endpoint.
With the advent of cellular immunotherapy, the role of transplantation for R/R DLBCL has been further refined. The 2022 National Comprehensive Cancer Network (NCCN) guidelines indicate that for patients who are not eligible for transplantation but willing to receive CAR-T therapy, axicabtagene ciloleucel (Axi-cel) with bridging therapy is recommended. The PILOT study was an open-label, single-arm, multicenter phase 2 study aimed at evaluating the efficacy and safety of lisocabtagene maraleucel (Liso-cel) as second-line treatment for patients with R/R LBCL who were not planned for hematopoietic stem cell transplantation (HSCT). The final analysis results presented at the 2023 ASH annual meeting were consistent with the primary analysis, showing that Liso-cel treatment resulted in high CR rates, prolonged DOR, and durable CR in patients with R/R LBCL who were not planned for HSCT. The median overall response duration was 23.3 months, and the median duration of response for patients achieving best complete response (bCR) was not reached. Similarly, the ALYCANTE study also evaluated the efficacy of Axi-cel as a second-line treatment for transplant-ineligible R/R DLBCL patients. The results presented at the 2023 EHA showed that at 3 months, the complete molecular remission (CMR) rate was 71% with Axi-cel, compared to an estimated 12% CMR rate with standard of care (SOC) in historical control studies. The ORR and CR rates were 90.3% and 79%, respectively. At a median follow-up of 12 months, the median PFS was 11.8 months, and the median OS was not reached, with a 12-month OS rate of 78.3%. The safety profile was manageable, and the efficacy and safety were consistent in patients aged ≥70 years.
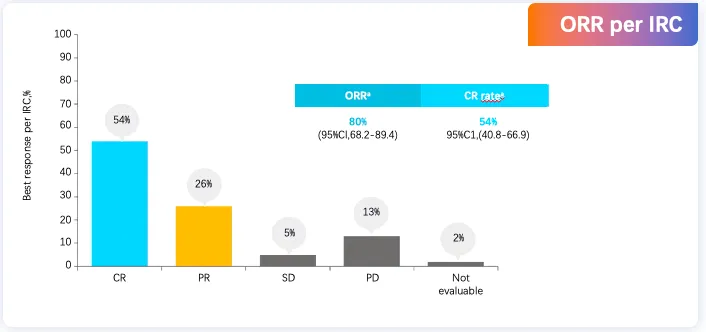
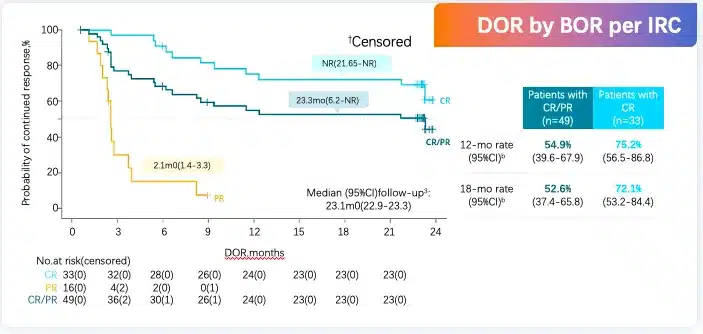
▲ Final analysis of the PILOT phase 2 study
CAR-T as second-line treatment – multiple issues to be addressed
There are still some pressing issues to be addressed regarding the use of CAR-T as a second-line treatment for DLBCL:
(1) The role of bridging therapy: Bridging therapy is very common in real-world studies, with 45%-53% of patients in the US and 78% of patients in Germany receiving bridging therapy. The bridging therapy rate was similar (63%) in the TRANSFORM study. Clinicians may still choose patients to receive bridging therapy based on disease severity (especially tumor volume and growth kinetics).
(2) Optimal treatment for chemotherapy-sensitive patients: Autologous stem cell transplantation (ASCT) can cure approximately 50% of chemotherapy-sensitive patients, and up to 40% of patients undergo ASCT in partial remission (PR). CAR-T therapy can still serve as a third-line treatment after ASCT relapse, with approximately 40% of patients achieving durable remission. If patients receive CAR-T therapy first without ASCT, it is currently unclear how many patients would still be eligible for ASCT or cured through ASCT after CAR-T failure. Additionally, for patients relapsing >12 months later, who are more likely to be chemotherapy-sensitive, it is unclear whether second-line CAR-T or salvage chemotherapy followed by ASCT is more appropriate.
(3) The enormous cost of CAR-T therapy.
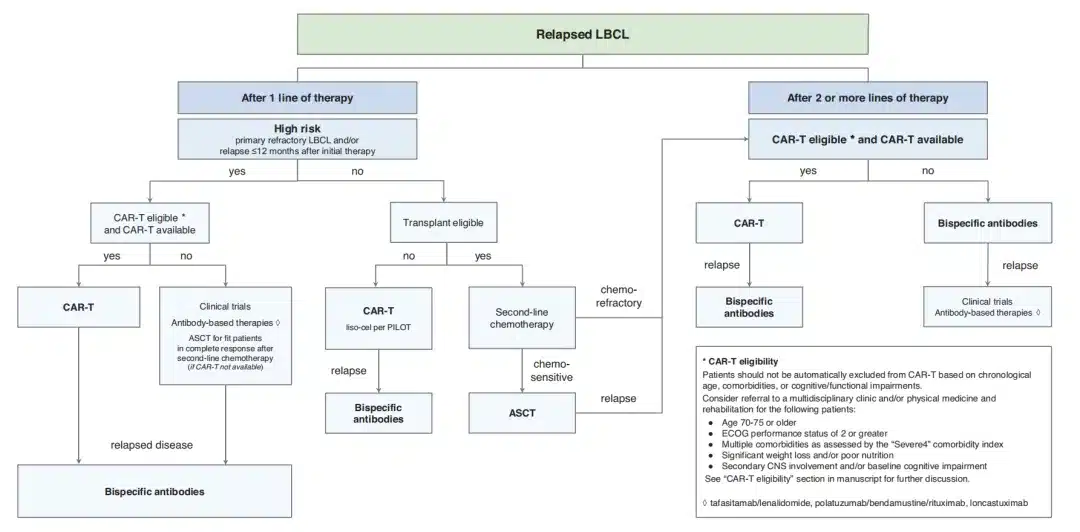
▲ Treatment algorithm for R/R DLBCL
Although anti-CD19 CAR-T cell therapy has been approved by the FDA as a second-line treatment for high-risk (primary refractory disease or relapse within 12 months of first-line therapy) LBCL, several practical issues need to be considered regarding its implementation, such as suitable histological subtypes, age, comorbidities, and tumor biology limitations, managing highly aggressive tumor behavior, whether holding or bridging/salvage therapy should be used before second-line CAR-T, and how to manage bridging therapy and whether to proceed with planned second-line CAR-T if the response to bridging therapy is good.
CAR-T optimization strategies – target innovation, enhanced functionality
Target innovation, enhanced functionality, reduced side effects, and universal cell therapy are the four major innovation trends in CAR-T therapy. Single-target CAR-T cells often encounter antigen escape and clonal evolution-driven antigen-negative relapse, while bi-specific CAR-T cells have the potential to overcome these limitations by more precisely targeting tumor cells, demonstrating better clinical efficacy and safety in various hematological malignancies and even solid tumors. Long-term follow-up results of the novel anti-CD20/CD19 bi-specific CAR-T (C-CAR039) in patients with R/R B-cell NHL showed that, with a median follow-up of 23.9 months, C-CAR039 exhibited a favorable safety profile and deep, durable responses, particularly in LBCL patients.
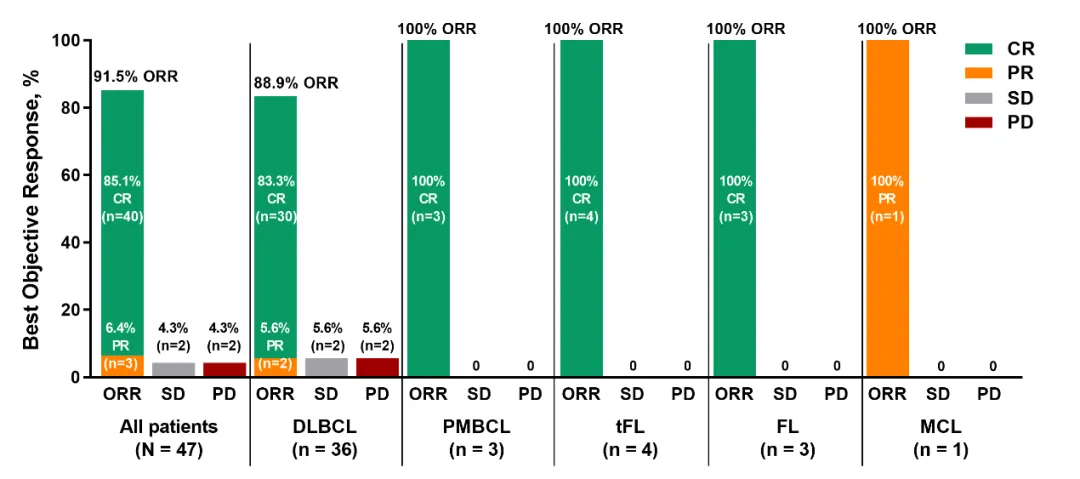
▲ Long-term follow-up results of the novel anti-CD20/CD19 bi-specific CAR-T (C-CAR039) in patients with R/R B-cell NHL
In terms of enhancing CAR-T cell functionality, Chinese scientists have made many contributions, including optimizing CAR structure, blocking immune checkpoint receptors, genetically modifying CAR-T cells, exploring combination therapies, optimizing ex vivo culture protocols, and CAR-T cocktail therapy. The first-in-human trial results of the fourth-generation 4-1BB CAR-T product HuCART19-IL18 for the treatment of R/R lymphoma were presented at the 2023 International Conference on Malignant Lymphoma (ICML). The study data showed that HuCART19-IL18 treatment could induce durable remissions in patients with R/R CD19+ NHL who had previously received second-generation anti-CD19 CAR-T therapy. Additionally, multiple studies have demonstrated the safety and efficacy of ASCT in combination with CAR-T therapy for B-NHL, particularly in patients with R/R DLBCL.
Summarize
In summary, lymphoma treatment has entered the era of cellular immunotherapy, with multiple approved anti-CD19 CAR-T therapies for R/R LBCL patients. Pivotal clinical trials and real-world studies have consistently shown significant efficacy of anti-CD19 CAR-T in R/R LBCL. To further enhance the therapeutic position and efficacy of CAR-T, future efforts should continue to explore more CAR-T targets, develop next-generation CARs and multi-target CAR-T cells, and combine CAR-T with other therapies. For high-risk LBCL patients, the optimal timing of CAR-T therapy is another area for future exploration.
References
[1] Johnson PC, et al. Leuk Lymphoma. 2020;1-7.
[2] Chavez JC. Ther Adv Hematol 2019, Vol. 10: 1–20.
[3] Roex G, et al. Pharmaceutics.2020;12(2):194.
[4] Ying ZT, Zhu J, et al. Cancer Med. 2020 Dec 31.
[5] Locke. Lancet Oncol. 2019;20:31.
[6] Jacobson. ASH 2020. Abstr 1187.
[7] Jaeger. ASH 2020. Abstr 1194.
[8] Abramson. Lancet. 2020;396:839.
[9] ASH 2023,Poster:4864
[10] Ying ZT, et al. ASCO 2022 Poster 7529.
[11] ASH 2023. Abstract 1032.
[12] ASH 2023. Abstract 6928.
[13] 2022 EHA P1182.
[14] 2023 ASH Oral 4886.
[15] N Engl J Med. 2022 Feb 17;386(7):640-654
[16] Lancet. 2022 Jun 18;399(10343):2294-2308.
[17] N Engl J Med 2022 Feb 17;386(7):629-639.
[18] NCCN Guidelines Version 2.2022.Diffuse Large B-Cell Lymphoma.
[19] 2023 ASH Oral 105.
[20] 2023 EHA S233.
[21] Nat Med. 2022 Nov 8. doi: 10.1038/s41591-022-02067-9.
[22] Lancet Haematol . 2023 Dec;10(12):e1006-e1015.
[23] Lancet Haematology,2022,9(12):e930-e941.
[24] Ping Li, Aibin Liang et al. ASH2023 Oral 1025.
[25] 2023 ICML.
[26] Cao Y, et al. Transplant Cell Ther. 2021 Nov;27(11):910.e1-910.e11.
[27] Wei Liu, et al; Blood 2020; 136 (Supplement 1): 2.
[28] Wang T .et al. Hematol Oncol. 2022 Oct;40(4):637-644.
[29] Wei J, et al. Signal Transduct Target Ther. 2022 Apr 11;7(1):101.
[30] Xue F,et al. J Oncol. 2022 Nov 29;2022:2900310.
Content Source:血液时讯